
How many people have heard this, or a similarly disempowering conclusion from their doctors?
- “Your pain is all in your head”
- “I think you’re just depressed”
- “We’ve done all of the tests, there’s nothing wrong with you”
For most people with fibromyalgia (FM), it takes a substantial amount of time to receive the proper pain-related diagnosis. In part, this is because fibromyalgia is still a poorly understood condition.
At a basic science level, our knowledge is growing rapidly. But progress has been much slower at the clinical level. Many have a profound distrust of a diagnosis based on symptoms alone when the symptom is pain, and basic research has not uncovered a test that would yield an unequivocal sign of pain.
What is Fibromyalgia?
Fibromyalgia is a disorder characterized by widespread musculoskeletal pain accompanied by fatigue, sleep, memory and mood issues. Researchers believe that fibromyalgia amplifies painful sensations by affecting the way your brain processes pain signals.
Symptoms sometimes begin after an emotional or physical trauma, surgery, infection or significant psychological stress. These do not likely cause fibromyalgia by themselves, but they are thought to trigger the onset of the disorder in people who are already susceptible to it. In other cases, symptoms gradually accumulate over time with no single triggering event.
Fibromyalgia patients hurt all over, yet we are not able to find any pathology in their muscles. Yet we must consider Fibromyalgia as a neuropathic pain syndrome manifested by painful muscles.
If you hurt all over and feel worn out, you may have fibromyalgia or chronic fatigue syndrome. Both are serious chronic illnesses that have specific criteria for diagnosis, but may be overlooked because blood tests are typically normal. The distinction between fibromyalgia and chronic fatigue syndrome is rather fuzzy, with up to 70 percent of patients meeting the diagnosis for both.
While many chronic pain syndromes mimic certain aspects of fibromyalgia, the 1990 American College of Rheumatology criteria identifies “fibro” patients with an 88 percent accuracy. This is just as accurate as blood tests for other medical conditions.
Fibromyalgia should not be viewed as a wastebasket diagnosis.
Why does Fibromyalgia hurt?
Researchers believe repeated nerve stimulation causes the brains of people with fibromyalgia to change. This change involves an abnormal increase in levels of certain chemicals in the brain that signal pain (neurotransmitters).
In addition, the brain’s pain receptors seem to develop a sort of memory of the pain and become more sensitive, meaning they can overreact to pain signals. Likewise, the “Brain’s” descending modulating systems are disturbed in Fibromyalgia causing the body to be oversensitive to even non-nociceptive stimulation.
Central Nervous System Research on Fibromyalgia
- Alterations in pain-related chemical transmitters have been reported in the spinal fluid (particularly substance P, nerve growth factor, serotonin, norepinephrine, and corticotropin releasing factor), (not in muscle)
- Elevated levels of pro-inflammatory cytokines, which are substances that form a communication link between your body’s immune and neurological systems, have been found by many research teams.
- Different brain imaging techniques by several research centers have all shown that the blood flow and metabolic processes in the brain are significantly disturbed.
- Almost all people with fibromyalgia report difficulties staying asleep (e.g., the natural processes in the brain that maintain sleep appear to be disrupted.)
- The autonomic nervous system, whose control center resides at the base of the brain to communicate with the CNS to regulate the peripheral tissues, is not functioning properly.
- Research on the primary pain control system in the spinal cord indicates that it is not filtering out or dampening incoming noxious signals from the peripheral tissues.
- Several research studies pertaining to memory function show people with fibromyalgia have an impaired ability to concentrate.
What are the symptoms of fibromyalgia?
Cognitive difficulties commonly referred to as “fibro fog” impairs the ability to focus, pay attention and concentrate on mental tasks. Fibromyalgia often co-exists with other painful conditions, such as:
- Irritable bowel syndrome
- Migraine and other types of headaches
- Interstitial cystitis or painful bladder syndrome
- Vulvodynia
- Temporomandibular joint disorders
- Post-traumatic stress disorder (PTSD)
Fibromyalgia Tender Points
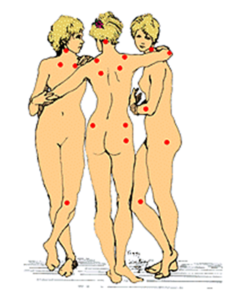
Routine lab tests do not detect the widespread pain of fibromyalgia. Instead, the diagnosis is made by a physical exam of pressure points.
When light pressure is applied to the surface of the muscles throughout the body, patients with fibromyalgia find this painful, especially at the specific tender point areas used for diagnosis.
To meet the fibromyalgia criteria, patients must have widespread pain in at least 11 of the 18 specified tender points in all four quadrants of the body for a minimum of three months.
The 18 sites used for the fibromyalgia diagnosis cluster around the neck, shoulder, chest, hip, knee, and elbow regions. The finger pressure that must be applied to these areas during an exam is just enough to cause the nail bed to blanch or become white.
What is the difference between tender points and trigger points?
For starters, 90 percent of the 18 predetermined tender points are actually myofascial trigger points. Trigger points are firm nodules that can often be felt in tight, rope-like muscles. Pressing on a trigger point hurts in the area and also shoots pain to other regions (non dermatomal radiation or referred pain), while pressing on a tender point is believed to only cause discomfort to the local area. The new, but still preliminary criteria for the fibromyalgia diagnosis were published in May of 2010.
In place of the tender point count, patients (or their physician) may endorse 19 body regions in which pain has been experienced during the past week. This number is referred to as the Widespread Pain Index (WPI) and it is one of the two required scores needed for a doctor to make a diagnosis of fibromyalgia.
The second part of the score needed to determine if a patient has fibromyalgia involves the evaluation of a person’s symptoms. The end result is a Symptom Severity score or SS score. The diagnosis is based on evaluating both the WPI score and the SS score. Overall, it takes into consideration the widespread nature of the pain and the other bothersome symptoms.
The greatest problem with the new criteria is that the authors do not state how severe the pain must be in order to check “yes” for that area. What if the pain is just a dull ache or intermittent? The criteria do not specify the intensity or quantity of pain that one must have in a given area over the past week to merit a “yes” answer.
Quantifying the symptoms for the SS score is even more vague. In fact, the control patients scored an average of 3 on a scale of 0 to 12, which is not far from the SS score required for fibromyalgia.
On the downside, is it possible these new criteria may greatly increase the number of patients diagnosed with fibro by diluting what is called “fibromyalgia?” Quite possibly, people with chronic, painful illnesses that do not involve widespread pain will meet the preliminary criteria for diagnosis. This could diminish the credibility of people with fibromyalgia.
The diagnosis of fibromyalgia may still be given in the usual clinical setting (e.g., in private practice) if widespread pain is present along with many of the commonly associated symptoms:
- Fatigue that is not relieved by rest
- Sleep disorder (or sleep that is unrefreshing)
- Irritable bowel (e.g., diarrhea, constipation, etc.)
- Chronic headaches (tension-type or migraines)
- Jaw pain (including TMJ dysfunction)
- Cognitive or memory impairment
- Numbness and tingling sensations
- Skin and chemical sensitivities
- Post-exertional malaise and muscle pain
- Morning stiffness (waking up stiff and achy)
Conditions that Mimic Fibromyalgia
- Low thyroid hormone levels (hypothyroidism)
- Vitamin D insufficiency
- Parathyroid disease (causing elevated blood calcium level)
- Muscle diseases causing muscle pain (such as polymyositis)
- Bone diseases causing bone pain (such as Paget’s disease)
- Elevated blood calcium (hypercalcemia)
- Infections diseases (such as hepatitis, Epstein Barr virus, AIDS)
- Cancer
Nervous System/Brain Chemistry
Studies have found that levels of several different chemicals important to brain and nervous system function are abnormal in people with fibromyalgia. These chemicals include:
- Serotonin, a neurotransmitter that helps regulate mood, sleep, and muscle contraction
- Tryptophan, an amino acid the body uses to make serotonin
- Norepinephrine, a hormone that regulates the body’s reaction to stress
- Substance P, a protein involved in transmitting pain signals from the nerves to the brain
Pain Medications for Fibromyalgia
You need both serotonin and norepinephrine reuptake inhibition for pain modulation.
Tricyclic Antidepressants
- Amitriptyline 10-25mg qhs
- Desipramine 10-25mg qhs (least anticholinergic)
- Doxepin 25mg qhs (most sedating)
- Imipramine 10-25mg/day
- Nortriptyline 10-25mg/day (best tolerated)
Non-Tricyclic antidepressants
- Venlafaxine (Effexor®) ≥ 150mg for norepinephrine
- Duloxetine (Cymbalta®) – 30mg/day advancing to 60-120mg/day
- Bupropion (Wellbutrin®) SR 150-300mg/day
- Trazadone (Deseryl®) 50-300mg/day (avoid in men)
Antispasmodics (muscle relaxants)
- Baclofen (Lioresal®)
- GABA receptor antagonist, descending pain modulation best for pain associated with spasticity, central pain mechanisms, 5mg tid to 15mg tid
- Tizanidine (Zanaflex®)
- Central modulation, Alpha-2 receptor inhibition, 1-2mg qhs titrating to 4-8mg qhs and 2-4mg bid, very sedating
- Carisoprodol (Soma®)
- Be careful, metabolized to meprobamate (barbiturate tranquilizer), high potential for dependence-addiction, seizures can occur 4-7 days after acute cessation from 4-6 tabs per day
Nonopioid Pain-Relieving Medications
- Acetaminophen
- Prototype nonsteroidal anti-inflammatory analgesic drugs
- Aspirin
- Choline magnesium trisalicylate
- Ibuprofen
- Naproxen
- Ketorolac tromethamine
- Cyclooxygenase-2 (COX-2) inhibitors
- Celecoxib only one left availabile
Anticonvulsants
- Gabapentin
- Pregabalin
- Topiramate
- Lamotrigine
- Clonazepam
- Carbamazepine
- Valproic acid
- Phenytoin
Corticosteroids
- Prednisone
- Dexamethasone
Membrane Stabilizers, Na+ Channel Blockers
- NMDA receptor blockade
- Ketamine, Dextromethorphan (100mg qid)
- GABA enhancers
Want to learn more about pain medicine? Explore our master and certificate programs in Pain Medicine, in partnership with the USC Keck School of Medicine.